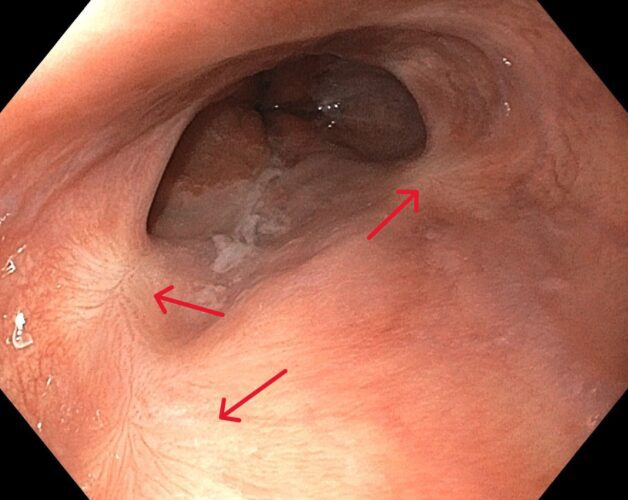
This 58-year-old woman with a history of chronic hepatitis C presents for a screening endoscopy after recently being diagnosed with liver cirrhosis. The following abnormality is noted in her lower esophagus. What is the name of this condition, and how is it caused?

This patient has esophageal varices (red), which are dilated esophageal veins. Varices can form in the esophagus, stomach, or rectum, and are most often caused by portal hypertension.
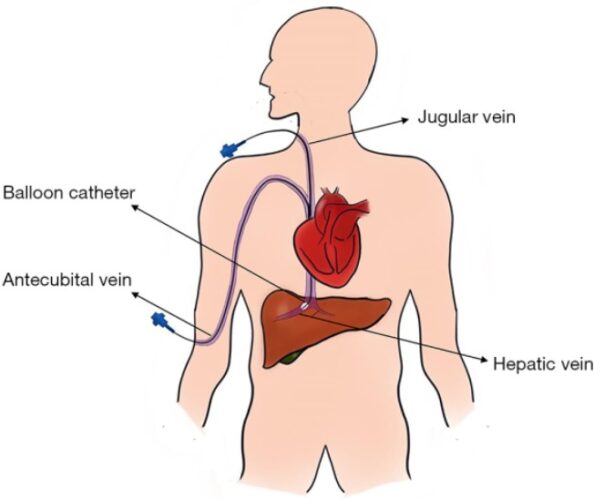
High portal pressures are typically a result of liver cirrhosis, but more rare causes of portal hypertension can include portal vein or splenic vein thrombosis, Budd-Chiari syndrome, schistosomiasis, and cardiac disease causing vascular congestion. Portal hypertension is defined as portal pressures above 5 mmHg, which can be measured using the hepatic vein pressure gradient (HPVG). The HPVG is measure by catheterization of the hepatic vein using a balloon tip cathter, under fluoroscopic guidance (second figure). Portal pressures greater than 10 mmHg are associated with the development of varices, and pressures greater than 12 mmHg are associated with variceal bleeding.
Varices are typically classified as large or small. During upper endoscopy, the esophagus should be insufflated when estimating variceal size. High risk features on endoscopy which increase the risk of variceal bleeding include large varices, the presence of the “red wale” sign (longitudinal red streaks), cherry red spots overlying varices, or diffuse erythema overlying the varices.
Sources: Lesmana CRA, Raharjo M, Gani RA. Managing liver cirrhotic complications: Overview of esophageal and gastric varices. Clin Mol Hepatol. 2020 Oct;26(4):444-460. doi: 10.3350/cmh.2020.0022. Epub 2020 Oct 1. PMID: 33053928; PMCID: PMC7641566.f. Available from https://pubmed.ncbi.nlm.nih.gov/33053928/
Xu G, Li F, Mao Y. Portal pressure monitoring-state-of-the-art and future perspective. Ann Transl Med. 2019 Oct;7(20):583. doi: 10.21037/atm.2019.09.22. PMID: 31807564; PMCID: PMC6861775. Available from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6861775/
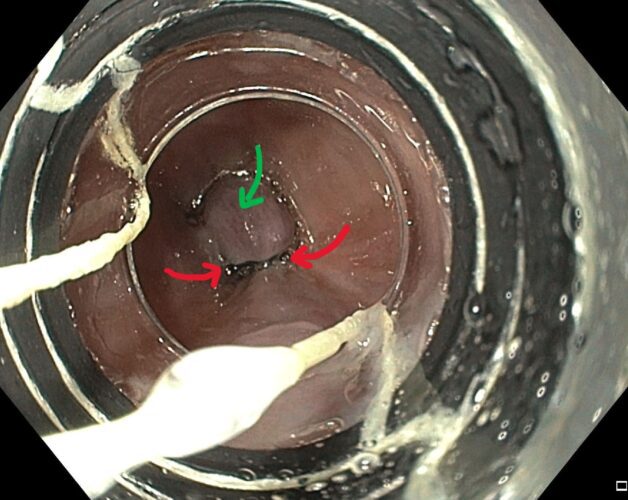
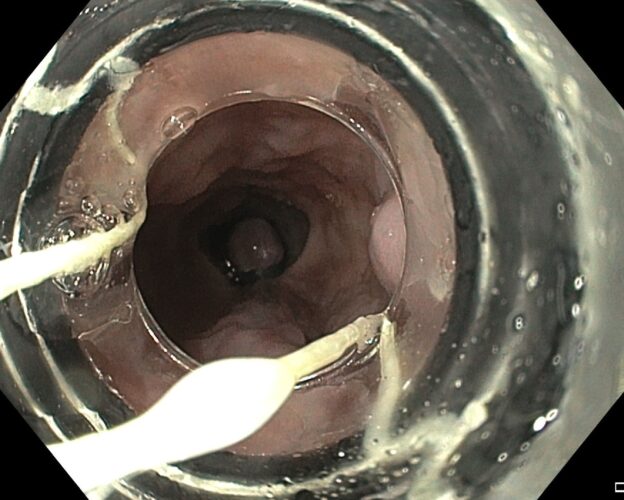
This patients’ varices were treated with band ligation, as shown in the images below. This technique involves attaching a short transparent cap to the tip of the endoscope, that facilitates the suction of the varices and application of an elastic band (red arrows), which cut off blood supply, causing it to shrink and necrose, before falling off after approximately one week. In the image below, the treated varix (green arrow) is shown.
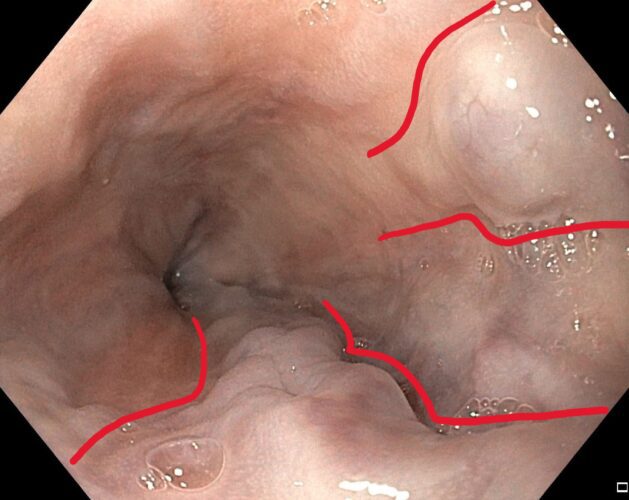
Three months later, a repeat upper endoscopy was performed, which demonstrated several healing sites from her banding (red) with interval resolution of her varices.