
This 45 year-old man with a four year history of Crohn’s disease was recently switched from a TNF-alpha inhibitor to an IL-12/IL-23 inhibitor, following treatment failure. A repeat colonoscopy for restaging revealed the following lesions – what explains this anatomical finding?
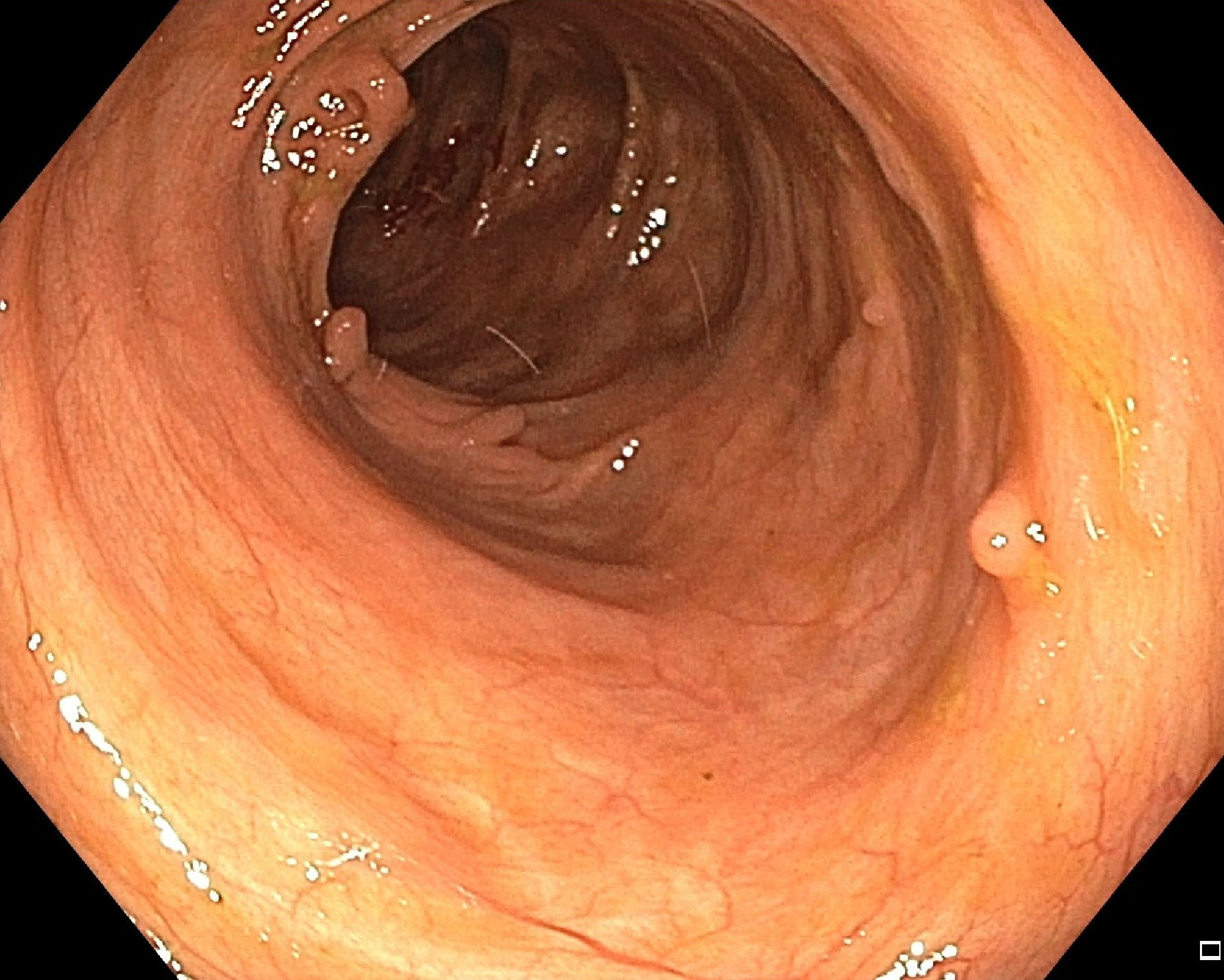

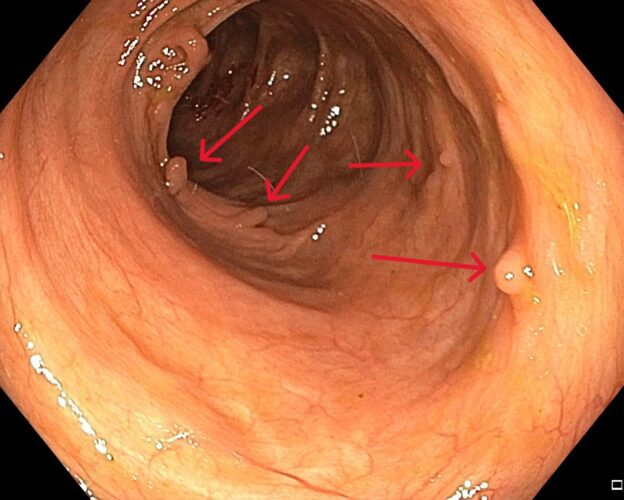
These lesions are called pseudopolyps (red arrows), which are non-neoplastic lesions formed due to hyperplastic healing following intense flares of IBD. They can appear in a variety of forms, from sessile to pedunculated, and their sizes vary, with lesions greater than 1.5 cm termed as giant pseudopolyps. Notably, they are more often found in ulcerative colitis than Crohn disease, with some authors reporting up to a twofold difference in prevalence.
These lesions are an indirect marker of previous episodes of severe inflammation, and patients with pseudopolyps are considered to be at an intermediate risk for colorectal cancer. While malignant transformation of the lesions themselves is extremely rare, the increased risk of colorectal cancer is attributed to previous severe inflammation.
From an endoscopic perspective, the surface of the pseudopolyps should be analyzed, but removal is not recommended, unless the lesion is large or causing obstruction, or if their is any clinical doubt about the diagnosis.
Source: Politis DS, Katsanos KH, Tsianos EV, Christodoulou DK. Pseudopolyps in inflammatory bowel diseases: Have we learned enough? World J Gastroenterol. 2017 Mar 7;23(9):1541-1551. doi: 10.3748/wjg.v23.i9.1541. PMID: 28321155; PMCID: PMC5340806. Accessilbe from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5340806/